Case One – January 2017
- 72 year old Caucasian male presented with acute onset of non-palpable, purpuric patches on left anterior proximal upper arm.
- Clinically thought to be a bruise in the ER.
- Did not resolve for ~2 months.
- Referred to dermatology

- Ecchymosis
- Malignant melanoma
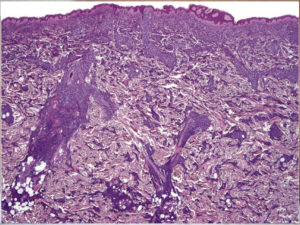
There is a dense perivascular, perifollicular & interstitial cellular lymphoid infiltrate, extending into subcutis. Areas of hemorrhage
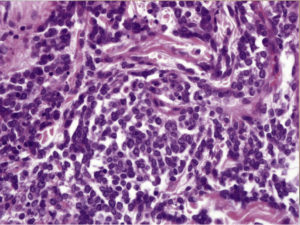
The infiltrate consists of a uniform population of cells with basophilic cytoplasm, round to oval nuclei, & small nucleoli.
Immunohistochemistry
- CD45+ (confirming lymphoid origin)
- Negative for mature B- and T-cell markers- CD3, CD5, CD7, CD20, CD79a.
- Negative for myeloid markers of AML like MPO, CD34, c-kit, lysozyme, CD33, CD68 (but can be TdT+)
- CD4+ CD8-
- CD56+
- CD123+ TCL-1+ (Marker of plasmacytoid dendritic cells)
Differential Dx
- Extranodal NK/T-cell lymphoma:
- This tumor is also CD56+, but CD4-.
- Also it is consistently positive for EBV; but BDCN is EBV negative.
- TCL-1 and CD123 are expressed almost exclusively in BDCN.
Blastic Plasmacytoid Dendritic Cell Neoplasm Facts
- BPDCN accounts for < 1% of all acute leukemia cases & 0.7% of cutaneous lymphomas.
- The male : female ratio is ≥ 3:1.
- Most patients are elderly (mean age of 67 years at presentation).
- Almost all cases have cutaneous lesions at presentation, & there is frequent involvement of BM & peripheral blood (60–90%) & LNs(40–50%), although virtually any organ can be affected.


Lesions can be solitary or multiple Affecting head, neck, trunk or extremities, Erythematous, violaceous or red-brown- nodules, tumors or plaques or Bruise-like lesions (as in our patient)
- The clinical course is aggressive with involvement of BM, PB, & other sites, and the development of cytopenia.
- Initial responses to treatment are relatively common, but most patients relapse within a short space of time.
- Poor prognosis with Median survival time only 12–14 months (estimated 5-year survival is 0%).
- In 10–20% of cases, BPDCN is associated with, or develops into, a myelodysplastic syndrome, myelomonocytic leukemia or acute myeloid leukemia.
What is this tumor, and why should I know about it?
- This is a very clinically aggressive tumor derived from the precursors of plasmacytoid dendritic cells.
- It has a high frequency of cutaneous, bone marrow & peripheral blood involvement with leukemic dissemination.
- In most cases the neoplasm is confined to the skin at presentation.
- However, leukemic spread after variable, usually short, periods of time is the rule, indicating that the primary cutaneous cases most likely represent “aleukemic” phase of leukemia cutis.
- Listed in the WHO book on Classification of Tumours of Hematopoietic and Lymphoid Tissues in section on Acute Myeloid Leukemia.
In the past known by various names like:
- Blastic NK-cell lymphoma
- Blastic NK-cell leukemia/lymphoma
- CD4+ CD56+ hematodermic neoplasm/tumor
- Important to remember this very aggressive lymphoma with a high frequency of leukemic dissemination.
- Skin lesions are most often the 1st presenting manifestation of the disease.
- Cutaneous lesions can be bruise-like or pigmented simulating melanoma.
- Histology can pose a diagnostic challenge.
- Because of its aggressive behavior it is important to correctly diagnose it in a timely fashion for proper clinical management.